Allergic rhinitis

It is defined as IgE mediated type I hypersensitivity reaction to any allergen such as pollen, pet hair, dust or mold. Inherited genetics and environmental exposures contribute to the development of allergies. Allergic rhinitis, eczema (atopic dermatitis), and asthma often occur together and are referred to as the atopic triad. Allergic rhinitis may also be associated with allergic pharyngitis, allergic conjunctivitis or urticaria. Environmental exposures such as air pollution and maternal tobacco smoking can increase an individual's chances of developing allergies.
Epidemiological studies demonstrate that the prevalence of allergic rhinitis has continued to rise over recent decades. However, the disease has so far been underestimated, as patients with less severe symptoms are less likely to seek medical advice and consult a doctor.
Globally, allergic rhinitis affects more than 400 million people, with
prevalence rates ranging from 10% to 30% in adults and over 40% in
children. Recent study done in Gandaki province of Nepal showed 23.8% allergic rhinitis out of 1810 patients having various types of allergic disease and 2.2 % had allergic rhinitis with bronchial asthma. This study reported non-juicy foods (96%), pollens (95%) and then juicy foods
(93%) being the most common allergens. In contrast to this in a study
done in Kathmandu the most common allergen found was mites (D. farina)
71.42% followed by D. Pteronyssinus 65.47% and Blomia species 64.28%.
Other positive aeroallergens found were house dust, cotton dust, wheat
dust, grain dust, paper dust, hay dust, pollens and fungi. Similarly, another study based on a skin prick test in patients presenting to a tertiary care hospital showed the dominance of house dust mites, dog and cat hair, pollen, and grasses.

Depending on the timing of the allergy, it can be seasonal or perennial. If it occurs in a certain season often as a result of exposure to pollen or cold it is called seasonal rhinitis. If it occurs throughout the year, it is called perennial allergic rhinitis.
Depending upon types of allergen it can be either occupational such as in wood workers or food allergy such as seafood, egg etc.
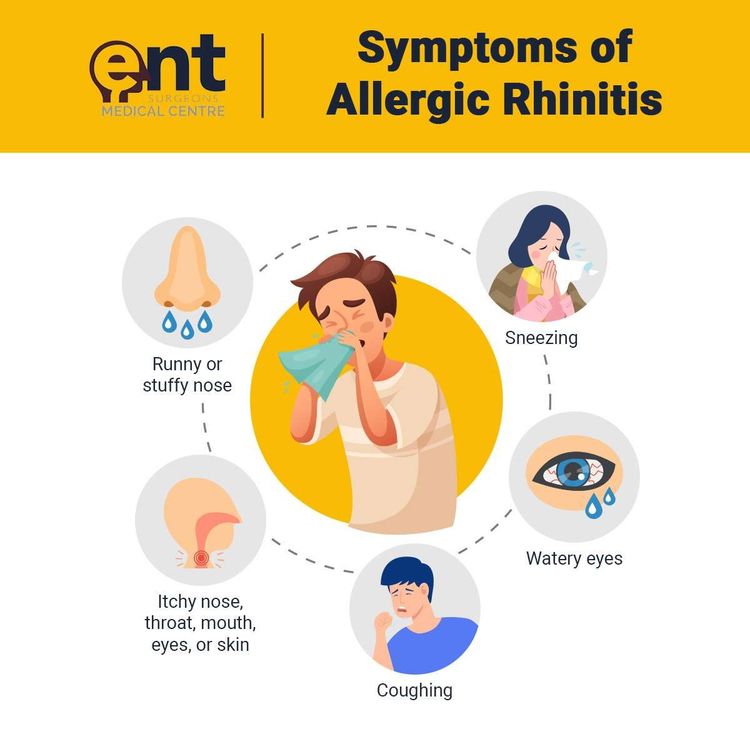
Symptom and signs include excessive sneezing, nasal discharge, nasal blockage and itching. It may be associated with itchy and watery eyes. There may be itchy throat with cough if there is allergic pharyngitis also. Symptoms often occur within minutes of exposure to allergen.
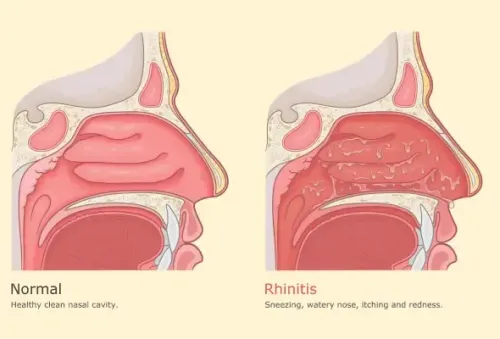
There will be clear (mucoid) nasal discharge with boggy inferior turbinate (Fig.1). In the initial phase the mucosa of the nasal cavity will be congested. Whereas in the chronic stage, the mucosa becomes pale and granular. Due to frequent rubbing of nose there will be a transverse crease on the dorsum, called allergic salute (Fig.2). In addition to these there will be redness of eyes with swollen eyelids known as Dennie–Morgan folds and lower eyelid venous stasis (rings under the eyes known as 'allergic shiners') (Fig.3). Patients may also complain of blocked ears due to Eustachian tube obstruction leading to middle ear effusion.
Diagnosis is typically based on a combination of symptoms.
The symptoms of allergic rhinitis resemble those of the common cold. However, they often last for more than two weeks and do not include a fever. In case of common cold (coryza) which is viral in cause lasts only for a few days and is associated with fever and malaise.
Another differential diagnosis is intrinsic rhinitis, which is mainly due to parasympathetic over activity associated with emotional changes and usually occurs in females. In such case inferior turbinate will be boggy and bluish in color.
Allergy tests such as patch test, skin prick test, scratch test or blood tests for allergen-specific IgE antibodies, RAST can help to identify the allergen. However, allergy test is not definitive. At times, these tests can reveal positive results for certain allergens that are not actually causing symptoms, and can also not pick up allergens that do cause an individual's symptoms.
Antihistamines such as fexofenadine, loratadine, desloratadine, cetirizine, levocetrizine, ebastine are available in the market.
Mast cell stabilizer - sodium cromoglycate.
Leukotriene receptor antagonists such as montelukast.
Intranasal steroid spray- Mometasone, fluticasone, budesonide.
Topical decongestants may also be helpful in reducing symptoms such as nasal congestion, but should not be used for long periods, as it can lead to a rebound nasal congestion called rhinitis medicamentosa.
Nasal saline irrigation with saline water may have benefits in relieving the symptoms of allergic rhinitis
Oral steroids – in severe cases, especially if associated with bronchial asthma, may be necessary.
Immunotherapy also called desensitization, is often effective and is used when first line treatments fail to control symptoms. It is done by exposing patient to larger and larger amounts of allergen. The allergen can be given as subcutaneous injection or as a sublingual tablet or drop.
Early exposure to allergens might reduce the risk of developing these specific allergies. Avoidance of allergens is the best preventive measure. These methods include not having pets, carpets or old furniture at home, keeping the home dry and using mask while handling old papers, cloths and cleaning the rooms.
Gaindakot-10, Nawalpur
+977 78 502004
info@timepharma.com
10 am to 5 pm
© 2025 Time Pharmaceuticals. All rights reserved.